
Introduction
Psoriasis is an autoimmune-driven skin condition characterized by rapid skin cell turnover, leading to scaling, redness, and chronic inflammation. Light therapy has a long established place in psoriasis management - narrowband UVB phototherapy has decades of clinical evidence as a first-line treatment for moderate-to-severe psoriasis.
LED light therapy (red, blue, or combined wavelengths) is a different category from clinical phototherapy - it uses non-UV visible and near-infrared light. The evidence for LED therapy in psoriasis is growing but more limited than clinical phototherapy. This guide covers what is established, where LED therapy fits, and what realistic expectations look like.
Key Takeaways
- Narrowband UVB remains the most clinically established phototherapy for psoriasis - LED therapy is not a replacement
- Red light therapy (630-670nm) has evidence for anti-inflammatory effects and skin quality support that may benefit psoriasis-affected skin
- Blue light therapy (415nm) has some evidence for antimicrobial and anti-inflammatory effects relevant to psoriatic plaques
- At-home LED devices offer consistent supplement to treatment but operate at lower irradiance than clinical systems
- LED therapy is most appropriate as a complementary tool for mild-to-moderate psoriasis or between clinical treatment cycles, not as a primary treatment for severe cases
- Any change to psoriasis management should be discussed with a dermatologist
Understanding the Light Therapy Landscape for Psoriasis
Not all light therapy for psoriasis is the same. The three main categories differ significantly:
| Treatment | Wavelength | Mechanism | Evidence strength |
|---|---|---|---|
| Narrowband UVB (NB-UVB) | 311-313nm | Immunosuppressive effect on T cells in skin, reduces inflammatory cascade | Decades of strong clinical evidence; first-line treatment |
| PUVA (psoralen + UVA) | 320-400nm | Psoralen drug + UVA light; photochemical immunosuppression | Strong evidence; more side effects than NB-UVB |
| Red LED (630-670nm) | Visible red | Anti-inflammatory photobiomodulation; cellular energy support | Growing evidence; smaller, newer trials |
| Blue LED (415nm) | Visible blue | Antimicrobial, some anti-inflammatory effects | Limited but emerging evidence for psoriasis |
Red Light Therapy
Multiple studies on photobiomodulation for inflammatory skin conditions have shown:
- Reduction in pro-inflammatory cytokines (TNF-a, IL-6, IL-1b)
- Improved skin barrier function
- Reduced redness and inflammatory response in treated areas
For psoriasis specifically, red light's anti-inflammatory mechanism is relevant because psoriasis is primarily driven by immune dysregulation and chronic inflammation. Research on red light wavelengths for skin in this specific indication is smaller-scale than the broader photobiomodulation literature, but the mechanistic basis is coherent.
Blue Light Therapy
Blue light at 415nm has antibacterial and anti-inflammatory effects studied primarily in acne contexts. Some researchers have examined it for psoriasis-related inflammation, with preliminary positive findings. The evidence base is less developed than for red light in this application.
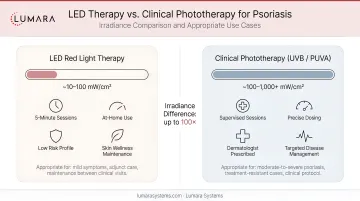
Clinical Phototherapy vs At-Home LED
The key distinction is irradiance. Clinical NB-UVB systems deliver precise UV doses at calibrated irradiance levels. At-home LED devices deliver non-UV light at consumer irradiance levels - lower than clinical systems. This affects how quickly results accumulate.
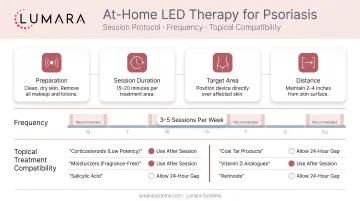
How to Use LED Light Therapy for Psoriasis at Home
Positioning
Apply the device over affected areas with the device at the manufacturer's recommended distance (typically 6-12" for panels, direct contact for pad formats). Psoriasis most commonly affects elbows, knees, lower back, and scalp - body-contact pad formats work well for these areas.
Protocol
- 5-20 minutes per treatment area per session depending on device irradiance
- 3-5 sessions per week
- Consistent use over 4-8 weeks before assessing response
- Track plaque thickness, redness, and scale as objective markers
Compatibility with Other Psoriasis Treatments
Red LED therapy is generally compatible with topical psoriasis treatments (corticosteroids, vitamin D analogs, tar-based products). Apply topicals after light therapy sessions, not before. Do not use alongside active photosensitizing medications without dermatologist guidance.
Realistic Expectations
LED light therapy for psoriasis can reduce inflammation and support skin quality between or alongside clinical treatments. It is not a cure and is unlikely to clear moderate-to-severe psoriasis on its own.
The most realistic application:
- Mild plaque psoriasis where clinical phototherapy is not available or not appropriate
- Maintenance between clinical treatment cycles
- Support for skin quality and inflammation reduction in combination with topical management
For significant, widespread, or rapidly worsening psoriasis, dermatology consultation and clinical phototherapy remain the more established approach.
Which Lumara Device Fits This Application
For body-surface psoriasis (elbows, knees, lower back, legs), a body-contact flexible pad or panel format provides the most practical coverage:
Lumara Pad: Red, near-infrared, and far-infrared wavelengths in a flexible body-contact format. Multiple sizes available. Best for direct-contact treatment of affected body areas.
Illuminate V2: 660nm red light panel with 1,200 cm2 coverage. Panel format suited for positioning over larger body areas or positioning against the back.
For facial or scalp psoriasis, a facial mask format is less commonly appropriate for psoriasis given the chronic nature of the condition and medical management requirements - consult your dermatologist about facial phototherapy.
Frequently Asked Questions
Does LED light therapy help psoriasis?
Red light therapy for psoriasis at 630-670nm has evidence for anti-inflammatory effects relevant to psoriasis. It is more appropriately used as a complement to medical treatment than a standalone therapy for moderate-to-severe psoriasis.
Is LED therapy the same as phototherapy for psoriasis?
No. Clinical phototherapy for psoriasis uses narrowband UVB (311-313nm) - UV light with decades of clinical evidence. LED therapy uses visible red or blue light (415-670nm) - different wavelengths with different mechanisms and different evidence depth.
How often should I use LED therapy for psoriasis?
3-5 sessions per week for at-home use. Assess after 4-8 weeks of consistent use to determine response. Adjust frequency based on skin tolerance.
Can red light therapy replace clinical psoriasis treatment?
No. Clinical phototherapy (NB-UVB) and dermatological treatments remain the primary standard of care for moderate-to-severe psoriasis. LED therapy is most appropriate as a complementary supportive approach.
Should I talk to my dermatologist before starting?
Yes. Psoriasis management is individualized and should involve dermatological guidance. Any addition to your treatment routine should be discussed with the treating physician.
LED Therapy as Part of a Broader Psoriasis Management Approach
LED light therapy has a legitimate place in psoriasis management - not as a primary treatment, but as a consistent anti-inflammatory tool that supports skin quality between or alongside clinical care.
For body-focused psoriasis applications, Lumara's Pad - flexible format, red/NIR/FIR wavelengths, multiple sizes - is built for the direct-contact body use that psoriasis treatment on elbows, knees, and back requires.


