Introduction
Psoriasis is a chronic autoimmune skin condition producing scaling plaques and inflammation. Light therapy has a long-established place in psoriasis management - but the category of "light therapy" covers a wide range of wavelengths, mechanisms, and evidence levels. Understanding the differences between clinical phototherapy and consumer LED devices matters for setting accurate expectations.
Key Takeaways
- Narrowband UVB phototherapy (311-313nm) is the gold standard for psoriasis among light therapy approaches - decades of clinical evidence, widely prescribed
- Consumer red LED therapy (630-670nm) has anti-inflammatory evidence relevant to psoriatic plaques, but different mechanism and evidence strength than clinical phototherapy
- Consumer LED devices are appropriate as a complementary tool for mild-to-moderate plaque psoriasis, particularly for maintenance between flares
- Red LED therapy is not a substitute for clinical phototherapy or systemic treatment in moderate-to-severe psoriasis
- Consistent body-area coverage matters: flexible pads work better than panels for elbows, knees, and lower back where psoriasis commonly presents
The Light Therapy Landscape for Psoriasis
Clinical Phototherapy (Narrowband UVB)
Narrowband UVB at 311-313nm is the most established phototherapy approach for psoriasis. It works by suppressing the T-cell activity driving autoimmune skin inflammation. Decades of controlled trials support its efficacy for moderate-to-severe plaque psoriasis.
Clinical phototherapy requires physician prescription and clinic access. It uses UV wavelengths that are not produced by consumer LED devices. For a breakdown of how red light panels compare to mask formats, see that guide for device format considerations.
Consumer Red LED Therapy (630-670nm)
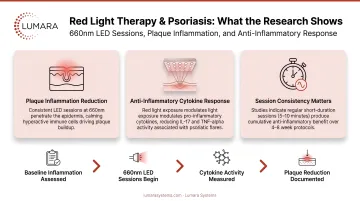
Red light at 630-670nm has documented anti-inflammatory effects - reducing pro-inflammatory cytokines (TNF-a, IL-6, IL-1b) - that are relevant to the chronic inflammation underlying psoriatic plaques. Wavelength precision matters for achieving these cellular effects. The mechanism is different from UVB and the evidence base is smaller, but the anti-inflammatory pathway addresses a real component of psoriasis.
What the Research Shows for Red LED Therapy
Studies on red light for inflammatory skin conditions show:
- Reduction in plaque thickness and erythema scores with consistent treatment
- Anti-inflammatory cytokine reductions in treated tissue
- Improvements in overall plaque appearance with 4-8 weeks of consistent sessions
These results are smaller in magnitude than clinical UVB phototherapy trials. Red LED therapy for psoriasis is more accurately positioned as a supportive tool - particularly for:
- Mild plaque psoriasis where clinical phototherapy is not prescribed
- Maintenance during remission to extend clear intervals
- Adjunct use alongside topical treatments
How to Use Red Light Therapy for Psoriasis
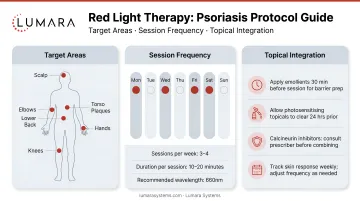
Target Areas
Psoriasis most commonly affects elbows, knees, lower back, and scalp. For device-based treatment:
- Elbows and knees: Use a flexible pad or small panel positioned directly against the plaque area
- Lower back: Larger flexible pad (12x30" or 20x30") covers this area in a single session
- Scalp psoriasis: Panel-based sessions with appropriate positioning; near-infrared may be more relevant for scalp tissue depth
Protocol
- 10-20 minutes per treatment area per session
- 3-5 sessions per week
- Consistent use over 4-8 weeks before assessing improvement
- Continue as maintenance if improvement is achieved
- Always use appropriate eye protection during sessions
Complementary Use with Topicals
Red light therapy is compatible with topical psoriasis treatments (corticosteroids, vitamin D analogs). Apply topicals after light therapy sessions - not before, as they can block light penetration. Discuss any treatment combinations with your dermatologist.
Realistic Expectations
Red LED therapy for psoriasis produces real anti-inflammatory effects, but:
- Results are typically less dramatic than clinical UVB phototherapy
- Psoriasis is a chronic autoimmune condition - any approach manages, not cures
- Individual response varies significantly based on plaque type, disease severity, and other treatment factors
- Stopping treatment typically leads to return of symptoms over time
Red light therapy is most valuable for users who want a consistent between-flare maintenance tool or a supplementary option for mild psoriasis that does not require clinical phototherapy.
Anyone with moderate-to-severe psoriasis should be under dermatological care, with red light therapy as one element of a broader management plan. Early research also suggests potential benefits for psoriatic arthritis and joint inflammation. The difference between infrared and red light therapy is worth understanding if you are considering near-infrared wavelengths for deeper tissue involvement.
Device Format for Psoriasis
For the common psoriasis locations (elbows, knees, lower back), flexible pads that can be placed directly against the affected area provide more consistent coverage than panels.
Lumara's Pad - available in multiple sizes, with red, near-infrared, and far-infrared wavelengths - is suited to direct-contact body-area use for the large joints and lower back areas where psoriasis commonly presents.

Frequently Asked Questions
Does red light therapy help psoriasis?
Red LED therapy has anti-inflammatory evidence relevant to psoriatic plaques. It is most appropriate as a complementary tool for mild-to-moderate psoriasis or between-flare maintenance. It is not equivalent to clinical UVB phototherapy for moderate-to-severe disease.
Is red light therapy or narrowband UVB better for psoriasis?
For moderate-to-severe psoriasis, clinical narrowband UVB has stronger evidence. For mild psoriasis or maintenance use, consumer red LED therapy provides meaningful anti-inflammatory support with convenient at-home access.
How long does it take to see results?
4-8 weeks of consistent use (3-5x/week) is the typical assessment window. Results vary by plaque severity and individual response.
Should I see a dermatologist for psoriasis?
Yes. Anyone with psoriasis should have a dermatology evaluation to understand their disease type and severity and develop an appropriate management plan. Red light therapy can be part of that plan.
Anti-Inflammatory Support for Psoriasis Management
Red light therapy is a legitimate complementary approach for psoriasis - not a cure, but a consistent anti-inflammatory tool that fits into a management routine as part of a consistent, non-invasive support routine.
For body-area psoriasis at elbows, knees, and lower back, Lumara's Pad for targeted body-area light therapy - flexible direct-contact coverage for elbows, knees, and lower back, with multiple sizes and a 3-year warranty - provides the consistent body-area coverage that makes ongoing use practical.