Introduction
Post-inflammatory hyperpigmentation (PIH) is one of the most common skin concerns - and one of the most frustrating. It appears when inflammation triggers excess melanin production in skin, leaving dark marks that can persist for months or years after the original trigger (acne, injury, eczema) has healed.
This guide covers the evidence-backed approaches to PIH treatment, where different light wavelengths fit into a management routine, and how to build a consistent protocol.
Key Takeaways
- PIH is triggered by inflammation activating melanocytes, causing localized melanin overproduction
- Prevention (avoiding or managing inflammation triggers) is the most effective long-term strategy
- Active treatment requires consistent use of ingredients that address melanin production or surface pigmentation
- Daily SPF is non-negotiable - UV exposure significantly worsens PIH
- Green light therapy at 525nm may support the appearance of uneven tone and discoloration as part of a consistent skincare routine
- Results from any PIH treatment require weeks to months of consistent use; there are no fast fixes
What Causes Post-Inflammatory Hyperpigmentation
PIH is the result of a normal skin defense mechanism misapplied. When skin is inflamed, melanocytes (melanin-producing cells) are activated as part of the response. In some cases - particularly in deeper skin tones - this activation leads to excess melanin deposition that persists after the inflammatory trigger resolves.
Common PIH triggers:
- Acne breakouts (the most common trigger)
- Eczema and dermatitis flares
- Physical trauma or wounds
- Post-procedure reactions (chemical peels, laser resurfacing)
- Insect bites and other skin injuries
The amount of PIH produced and how long it persists depends on skin tone (deeper tones produce more melanin generally), the severity of the original inflammation, and whether UV exposure is managed during healing.
Evidence-Backed Treatment Approaches
SPF (Non-Negotiable)
UV exposure activates melanocytes and will worsen PIH regardless of what other treatments you use. Daily broad-spectrum SPF 30+ is the foundation of any PIH protocol - not optional. This applies to all skin tones.
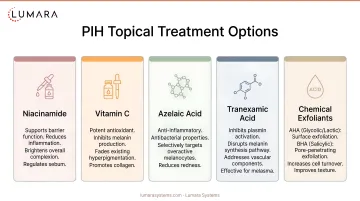
Topical Brightening Agents
Several topical ingredients have published evidence for reducing PIH:
Niacinamide (4-10%): Inhibits the transfer of melanin from melanocytes to skin cells. Well-tolerated across skin types. Can be used daily.
Vitamin C (L-ascorbic acid, 10-20%): Inhibits the enzyme tyrosinase, reducing melanin synthesis. Also provides antioxidant protection. Best used in the morning as part of your daily skincare routine.
Azelaic acid (10-20%): Both antimicrobial and melanin-inhibiting. Particularly relevant for PIH from acne. Available OTC and prescription.
Kojic acid: Natural tyrosinase inhibitor. Used at 1-4% in OTC formulations.
Tranexamic acid: Evidence-backed for melasma and PIH. Available in OTC serums and prescription formulations.
Hydroquinone: A potent pigment-focused ingredient that should generally be used under medical guidance. In the U.S., hydroquinone is not legally marketed as an FDA-approved OTC skin-lightening ingredient. Prescription strengths are available.
Chemical Exfoliants
AHAs (glycolic, lactic acid) and BHAs (salicylic acid) accelerate surface cell turnover, helping to shed melanin-containing cells and reveal less pigmented skin beneath. Consistent use over 8-12 weeks produces visible improvement. Chemical peels at higher concentrations can accelerate results for stubborn cases.
Use at night; always pair with daytime SPF.
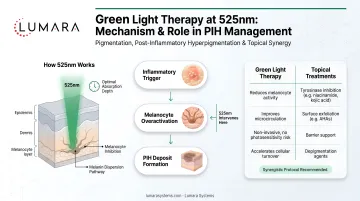
Where Green Light Therapy Fits
Green light at 525nm has a more direct relationship to pigmentation pathways than red light. The mechanism relevant to PIH:
- 525nm is absorbed by melanin in the skin
- This absorption may interfere with melanin synthesis processes and reduce overproduction signals in melanocytes
- Anti-inflammatory effects of green light may reduce the melanocyte activation that causes PIH in the first place
Green light therapy at 525nm can be positioned as a supportive skincare step for the appearance of uneven tone and discoloration, not as a standalone PIH treatment, but as a complement to topical protocols.
How it differs from red light (660nm): Red light at 660nm is more relevant for collagen, skin quality, and anti-inflammatory effects in recovery contexts. Green light has more specificity for melanin-related pigmentation concerns. Some patients also find that red light therapy skincare treatments complement their PIH protocols by reducing the underlying inflammation that triggers new pigment formation.
Lumara's Illuminate Green delivers 525nm green light across 1,800 LEDs in 5-minute sessions, FDA cleared, Made in USA.
| Spec | Detail |
|---|---|
| Wavelength | 525nm green light |
| LEDs | 1,800 |
| Session time | 5 minutes |
| Energy delivery | 6,000 joules per session |
| FDA status | FDA cleared |
| Made in | USA |
| Warranty | 3 years |
Building a PIH Management Routine
Morning:
- Gentle cleanser
- Vitamin C serum (10-20% L-ascorbic acid)
- Niacinamide serum
- Moisturizer
- SPF 30+ (essential)
Evening:
- Cleanse thoroughly
- Green light therapy session (5 minutes) on clean skin - if incorporating 525nm therapy
- AHA or BHA exfoliant (2-3x per week)
- Azelaic acid or tranexamic acid treatment serum
- Moisturizer
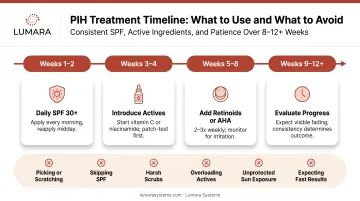
Timeline: Expect 8-12 weeks of consistent use before significant improvement in PIH appearance. Deep or established PIH may take 6 months or longer.
What Accelerates PIH and What to Avoid
Worsens PIH:
- UV exposure without SPF (most significant accelerant)
- Picking or manipulating affected skin
- Aggressive physical exfoliation
- Discontinuing actives before results are visible
Slows results:
- Inconsistent SPF application
- Skipping nights of active treatments
- Switching products too quickly before they have time to work
Frequently Asked Questions
How long does post-inflammatory hyperpigmentation take to fade?
Without treatment: 3-24 months depending on skin tone, depth of pigmentation, and UV exposure management. With consistent treatment (SPF + active ingredients): improvement typically visible at 8-12 weeks, with continued improvement over 6+ months.
What is the most effective treatment for PIH?
Daily SPF is the most important single intervention. Beyond that, niacinamide, vitamin C, azelaic acid, and tranexamic acid all have evidence for reducing PIH. Consistent use over months is required.
Does green light therapy help with PIH?
Green light at 525nm targets melanin-related pathways and has evidence for skin tone and discoloration appearance improvement. It is most effective as a complement to topical treatments rather than a standalone approach.
Can red light therapy help with PIH?
Red light at 660nm primarily supports collagen, skin quality, and anti-inflammatory recovery. Its benefit for PIH is indirect - by reducing inflammation, it may reduce the activation trigger for new PIH formation. Green light is more directly targeted at melanin-related pigmentation.
Is there a cure for post-inflammatory hyperpigmentation?
PIH will fade over time in most cases with appropriate management. "Cure" is not the right framing - it is a management process. Consistent SPF, active ingredients, and avoidance of UV without protection produce the most reliable long-term improvement.
Consistency, Protection, and the Right Wavelength
Post-inflammatory hyperpigmentation responds to consistent management: daily SPF without exception, active ingredients used for months not weeks, and supportive light therapy targeted at the pigmentation pathway.
Lumara's Illuminate Green - 525nm, 1,800 LEDs, 5-minute sessions, FDA cleared - is built for skin tone and discoloration appearance routines as part of a comprehensive PIH management approach.