
Introduction
Perioral dermatitis is one of the more frustrating skin conditions to manage. It looks like acne, but it does not always respond to the same treatments. It can flare unpredictably, worsen with common skincare products, and often return after clearing up. For people who have tried topical treatments without lasting results, blue light therapy is increasingly part of the conversation.
This guide covers what blue light therapy actually does at the skin level, what the evidence shows for inflammatory skin conditions, how it compares to red light therapy, and how to evaluate a device that fits into a practical routine.
Key Takeaways
- Blue light therapy at 415nm targets surface-level inflammatory activity and is used as part of skin clarity routines
- Perioral dermatitis is not purely bacterial - managing it often requires reducing inflammation alongside any antimicrobial approach
- Blue light has different depth and mechanism than red light; they are often used together for more complete coverage
- Device quality matters: wavelength accuracy, coverage, output, and FDA clearance are the criteria that separate effective devices from underperforming ones
- Lumara's Illuminate Blue delivers 415nm blue light across 1,800 LEDs at 6,000 joules per 5-minute session, FDA cleared, with a panel format built for consistent skin coverage
What Is Perioral Dermatitis
Perioral dermatitis is an inflammatory skin condition presenting as small red or flesh-colored bumps, typically around the mouth, nose, and chin. It is most common in women between their 20s and 40s, though it appears across age groups.
What makes it difficult to manage is that it does not have a single cause. Common contributing factors include:
- Prolonged use of topical steroids, including those in some skincare products
- Fluoride toothpaste contact with the perioral area
- Heavy occlusive moisturizers or makeup creating a barrier that traps irritants
- Hormonal fluctuations
- Stress and immune response changes
Because the triggers are varied, clearing perioral dermatitis often requires identifying and removing irritants alongside any treatment approach. Light therapy works alongside that management, not instead of it.
How Blue Light Therapy Works on Inflamed Skin
Blue light therapy at 415nm works through two main mechanisms that are relevant to inflamed, reactive skin like perioral dermatitis.
Antimicrobial Effect
Bacterial populations on the skin surface - including Cutibacterium acnes, the bacteria most associated with acne - produce compounds called porphyrins. When exposed to 415nm blue light, these porphyrins absorb the light energy, which disrupts the bacterial cell membrane. This is the same mechanism used in clinical blue light treatments for acne vulgaris.
Perioral dermatitis is not primarily a bacterial condition, but reducing surface bacterial load can lower one layer of inflammatory input, particularly in skin that is already sensitized.
Anti-Inflammatory Effect
Beyond antimicrobial activity, blue light at 415nm interacts with inflammatory signaling pathways in skin cells, helping to reduce localized inflammatory responses. For conditions where chronic low-grade inflammation is part of the picture - which perioral dermatitis often involves - this is the more directly relevant effect.
Penetration Depth
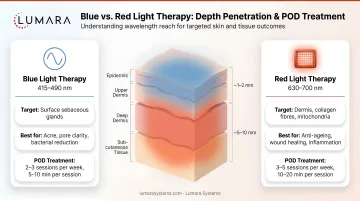
Blue light penetrates to approximately 1mm depth, which targets the epidermal layer and upper dermis. This is shallower than red light (which penetrates 4-5mm), meaning blue light is more concentrated at the surface. For a surface-presenting condition like perioral dermatitis, this depth profile is appropriate.

What the Evidence Shows
Most of the controlled research on blue light therapy is concentrated in acne vulgaris, where 415nm blue light has demonstrated meaningful reductions in inflammatory lesion counts across multiple studies. Perioral dermatitis shares several characteristics with acne: surface-level bacterial involvement, inflammatory activity, and skin barrier disruption.
Research on atopic dermatitis - another inflammatory skin condition - has also shown improvements in skin barrier function and inflammatory markers with blue light exposure.
Direct, large-scale RCT evidence for blue light specifically targeting perioral dermatitis is limited, as it is for most niche dermatological conditions. The more accurate framing is that blue light has an established research basis for surface-level inflammatory skin management, and perioral dermatitis falls within that category.
For users who want a more complete approach, blue light and red light are increasingly used in combination protocols. Blue light addresses surface-level bacterial and inflammatory activity; red light penetrates deeper and supports broader tissue-level anti-inflammatory responses. Combined, they address more of the inflammatory picture than either wavelength alone.
Blue Light vs Red Light for Perioral Dermatitis
Both wavelengths have a role. They are not competing approaches - they have different depth profiles and mechanisms.
| Factor | Blue Light (415nm) | Red Light (660nm) |
|---|---|---|
| Penetration depth | ~1mm (epidermal/upper dermal) | 4-5mm (dermal) |
| Primary mechanism | Antimicrobial, surface anti-inflammatory | Deeper tissue anti-inflammatory, cellular repair support |
| Best suited for | Surface bacterial load, reactive skin, early-stage inflammation | Deeper inflammation, skin barrier support, recovery routines |
| Used together? | Yes - combined protocols target more of the inflammatory cascade |
For perioral dermatitis, both can be part of a routine. Which to prioritize depends on where the skin is in its cycle - active flare versus recovery phase - and what the primary presenting concern is.
Lumara builds dedicated single-wavelength panels for both: Illuminate Blue at 415nm for blue-light routines, and Illuminate V2 at 660nm for red-light routines. Using them separately allows precise, consistent dosing at each wavelength, rather than relying on a panel vs mask format that blends both at reduced output.
What to Look for in a Blue Light Device
Most blue light devices on the market vary significantly in wavelength accuracy, coverage area, output, and build quality. The specs that matter most:
Wavelength Accuracy
415nm is the most studied wavelength for blue light skin applications. Devices that list a range (eg. "400-450nm") rather than a specific peak wavelength may not be delivering the full antimicrobial and anti-inflammatory effect of precise 415nm output. Look for devices that specify and verify their wavelength rather than approximating it.
Coverage Area
A small handheld device requires multiple passes to cover the perioral and perinasal area. A full panel format with consistent LED spacing delivers even coverage in a single session, reducing session time and variability.
Output and Energy Delivery
Higher LED count and energy output per session means more light energy delivered to tissue in each treatment. For meaningful skin-level effect, the device needs to deliver sufficient joules per session - not just emit light.
FDA Clearance
FDA clearance indicates the device has gone through the FDA's clearance pathway for its stated device category. It is a quality and safety signal, not a guarantee of individual outcomes.
Lumara Illuminate Blue: A 415nm Panel Built for Skin Routines
Illuminate Blue is Lumara's dedicated 415nm blue light panel. It is built for users who want a high-output, precisely wavelength-verified blue light device - not a low-cost consumer wand with inconsistent output.
| Spec | Detail |
|---|---|
| Wavelength | 415nm blue light |
| LEDs | 1,800 |
| Energy delivery | 6,000 joules per session |
| Session time | 5 minutes |
| Build | Ultra-slim, water-resistant |
| FDA status | FDA cleared, Class II medical device |
| Made in | USA |
| Eligible for | HSA/FSA |
| Warranty | 3 years |
| Claimed lifespan | 40,000 hours |
The panel format gives Illuminate Blue an advantage over smaller handheld blue light devices: 1,800 LEDs across a full panel surface means consistent coverage without repositioning, and 6,000 joules delivered in 5 minutes means the session is practical enough to sustain in a daily routine.
At 415nm, it is built around the wavelength most consistently referenced in blue light skin research - not a broad-spectrum approximation.

Building a Routine Around Blue Light Therapy
Manage Triggers First
Blue light therapy works best when used alongside the removal of known irritants. If topical steroids, fluoride toothpaste, or heavy moisturizers are triggering or sustaining the condition, reducing those inputs gives any treatment approach a better environment to work in.
Consistency Matters More Than Intensity
Blue light therapy for inflammatory skin conditions requires sustained, consistent sessions - not occasional high-intensity use. Daily or near-daily 5-minute sessions over 4-8 weeks is a more realistic baseline for evaluating results than a 2-week trial.
Combine with Red Light Where Appropriate
For skin that is in a recovery phase or dealing with deeper inflammation, alternating or combining with a red light routine addresses more of the inflammatory cascade. Lumara's Illuminate V2 (660nm) and Illuminate Blue (415nm) are designed to work independently or as part of a multi-wavelength routine.
Avoid Overloading the Skin
During active flares, keep the surrounding skincare routine minimal. Fewer products mean fewer potential irritants, and blue light therapy does not require any topical preparation to be effective.
Frequently Asked Questions
Does blue light therapy help with perioral dermatitis?
Blue light therapy at 415nm has an established research basis for surface-level inflammatory skin conditions, including those with a bacterial component. Perioral dermatitis involves surface inflammation and, in some cases, bacterial involvement, making it within the category where blue light is used. Direct large-scale trial evidence specific to perioral dermatitis is limited, but the mechanism is relevant to the condition.
How is perioral dermatitis different from acne?
Perioral dermatitis presents similarly to acne but has different underlying causes - it is more strongly linked to topical steroid use, heavy skincare products, and fluoride contact than to the sebaceous activity that drives acne. Standard acne treatments do not always resolve it, and some can worsen it.
Is blue light or red light better for perioral dermatitis?
Both have relevant mechanisms. Blue light targets surface bacterial activity and surface-level inflammation at ~1mm penetration. Red light supports deeper tissue-level anti-inflammatory responses at 4-5mm penetration. For perioral dermatitis, blue light addresses the more surface-presenting aspects; red light supports broader skin recovery. Combined use covers more of the inflammatory picture.
How long does it take to see results from blue light therapy?
Most research protocols run 4-8 weeks of consistent use before meaningful assessment. Individual results vary based on starting condition, trigger management, and routine consistency.
What wavelength should a blue light device use for skin?
415nm is the most researched wavelength for skin applications, particularly for antimicrobial and anti-inflammatory effects. Devices that specify a precise peak wavelength of 415nm rather than a broad range are more aligned with the research basis.
Is Lumara Illuminate Blue FDA cleared?
Yes. Illuminate Blue is FDA cleared as a Class II medical device. FDA clearance indicates the device has gone through the FDA's clearance pathway for its stated category - it is a quality and safety signal, not a guarantee of individual outcomes.
Can blue light therapy be used alongside other skincare treatments?
Yes, blue light therapy is generally compatible with most skincare routines. During active perioral dermatitis flares, keeping the routine minimal is recommended to reduce potential irritant exposure. Light therapy does not require topical products to work and can be used on clean skin.
Blue Light Therapy Is a Tool, Not a Fix
Perioral dermatitis responds to a combination of trigger removal and consistent anti-inflammatory support. Blue light therapy at 415nm fits into the support side of that equation: targeted, non-invasive, and compatible with a clean skincare routine.
The device you use matters. Wavelength accuracy, consistent coverage, output per session, and build quality determine whether a device delivers a clinically relevant dose or just emits light. Lumara's Illuminate Blue is built around those fundamentals - 415nm, 1,800 LEDs, 6,000 joules per 5-minute session, FDA cleared, Made in the USA.


