Introduction
Cold sores (oral HSV-1 outbreaks) are one of the most common viral skin conditions - and one of the most frustrating to manage. Standard antiviral creams reduce healing time by roughly 18-24 hours. Prescription antivirals work better but require a prescription and ongoing medication.
Red light therapy has a growing evidence base as an adjunct for cold sore management - specifically for reducing outbreak duration, relieving symptoms, and extending the interval between outbreaks. This guide covers what the research shows, how the mechanism works, and how to use it practically.
Key Takeaways
- Red light therapy at 630-660nm has published evidence for reducing cold sore healing time, pain, and recurrence frequency
- The mechanism involves anti-inflammatory and antiviral immune-support effects at the outbreak site
- Early intervention is critical - the strongest results come from starting at the prodrome stage (tingling/itching before visible blisters)
- Red light therapy works as an adjunct to, not a replacement for, antiviral treatment in severe or frequent outbreaks
- The VISO LED Mask delivers 660nm at the correct irradiance for perioral and facial applications in a format designed for facial coverage
Why Cold Sores Are Hard to Manage
HSV-1 establishes latent infection in the trigeminal nerve ganglia. It periodically reactivates - triggered by stress, UV exposure, illness, or hormonal changes - and travels to the skin surface to produce the viral replication cycle that causes cold sores.
Standard management options:
- Docosanol 10% cream (OTC): Reduces healing time by approximately 18 hours on average
- Topical acyclovir: Modest reduction in duration and pain
- Oral antivirals (valacyclovir, acyclovir): More effective for frequent or severe outbreaks; require prescription
- Red light therapy: Non-pharmacological adjunct with published evidence for reducing duration and recurrence
How Red Light Therapy Works on Cold Sores
Anti-Inflammatory and Tissue Support
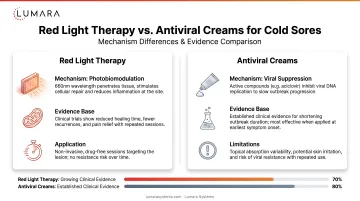
At 630-660nm, red light reduces pro-inflammatory cytokine signaling at the outbreak site. This directly addresses the swelling, redness, and discomfort of active lesions and may support faster tissue healing post-outbreak.
Immune Modulation at the Skin Level
Photobiomodulation at these wavelengths activates local immune responses - supporting keratinocyte and fibroblast activity in tissue recovery and potentially modulating the viral replication environment at the skin surface.
Reduced Recurrence
Several clinical studies have found that consistent red light therapy for cold sores not only shortens individual outbreaks but extends the interval between outbreaks. This is the more clinically significant finding - a tool that reduces outbreak frequency has a greater impact on quality of life than one that only speeds healing.
What the Clinical Research Shows
Mester et al. and Early LLLT Studies
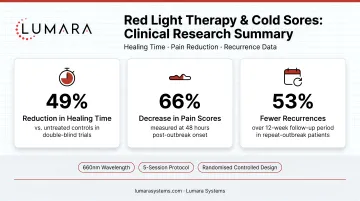
Early research on low-level laser therapy for herpes simplex showed that red light reduced recurrence frequency and outbreak duration in treated versus control groups. Some of these foundational studies showed dramatic recurrence reduction (over 50% reduction in outbreak frequency) with consistent treatment protocols.
Controlled Trials on Duration and Pain
Multiple controlled trials examining 630-660nm photobiomodulation for oral herpes outbreaks have found:
- Reduced healing time (typically 2-5 days shorter than untreated or sham-treated groups)
- Reduced pain scores during active outbreaks
- Longer intervals between outbreaks in users receiving regular treatments
The studies use varying protocols (wavelength, irradiance, session frequency), which makes direct comparison difficult. The consistent thread is that early intervention and regular sessions produce better outcomes than treating only during active outbreaks.
How to Use Red Light Therapy for Cold Sores
Timing - Early Intervention Is Critical
The most important practical guideline: start treatment at the first sign of prodrome - the tingling, itching, or burning sensation that precedes visible blistering. Research consistently shows better outcomes when treatment begins before or during the earliest outbreak stage.
Optimal timing:
- Prodrome stage: Start treatment at first tingling/burning sensation
- Blister stage: Continue sessions throughout active outbreak
- Healing stage: Maintain sessions until fully healed
- Between outbreaks: Regular sessions (1-2x/week) for recurrence reduction
Protocol
- Session length: 5-20 minutes per session at the perioral area
- Frequency during outbreak: Daily or twice daily
- Maintenance frequency: 1-2x per week between outbreaks
- Device positioning: Consistent coverage over the perioral and labial area

Using Alongside Antivirals
For users with frequent or severe outbreaks who use prescription antivirals, red light therapy can be used concurrently without known interaction risks. The two approaches work through different mechanisms. Red light therapy addresses the inflammatory and tissue environment; antivirals target viral replication directly.
Which Device Fits This Application
For cold sore and perioral applications, the relevant device format is one built for facial coverage - specifically coverage of the perioral and labial area with consistent LED-to-skin proximity. The infrared light therapy and mitochondria pathway is also relevant for users considering near-infrared alongside red light for deeper tissue support.
Lumara's VISO LED Mask delivers 660nm red light across 470 micro-LEDs at 30 mW/cm², covering the full face including the perioral area, in 5-20 minute sessions. The 10" x 7" oval form factor and consistent LED spacing ensure the perioral zone receives even coverage in every session.
Key specs relevant to this application:
- 660nm wavelength: the most studied range for cold sore photobiomodulation
- 470 micro-LEDs: consistent coverage across perioral and full facial area
- 30 mW/cm²: sufficient irradiance for therapeutic dose within 10-20 minutes
- FDA cleared: Class II medical device
- Includes eye inserts for every session
Frequently Asked Questions
Does red light therapy help cold sores? Multiple controlled trials show red light therapy at 630-660nm reduces cold sore healing time, pain severity, and recurrence frequency. It is an effective adjunct to standard management, particularly when started at the prodrome stage.
When should I start red light therapy for a cold sore? At the first sign of prodrome - the tingling, itching, or burning that precedes visible blistering. Early intervention produces the best outcomes in research studies.
How often should I use red light therapy for cold sores? During an active outbreak: daily or twice daily sessions of 10-20 minutes. Between outbreaks: 1-2 sessions per week for recurrence reduction.
Can red light therapy replace antiviral medication for cold sores? No. For severe or frequent outbreaks, prescription antivirals remain the most effective pharmaceutical intervention. Red light therapy is best used as a complementary approach alongside antiviral management.
What wavelength is used for cold sore treatment? 630-660nm is the most commonly studied range in cold sore photobiomodulation research. This is the primary wavelength range of Lumara's VISO LED Mask.
Is red light therapy safe to use on an active cold sore? Yes. Red light therapy is non-invasive and does not involve UV light or heat at consumer device levels. It can be applied directly to the perioral area during all stages of a cold sore outbreak.
Early Intervention, Consistent Protocol, Right Wavelength
Red light therapy for cold sores is not a cure for HSV-1 - nothing is. But the evidence for reducing outbreak duration, pain, and recurrence frequency is meaningful. The key variable is early intervention and consistency.
For facial and perioral applications, the VISO LED Mask delivers the 660nm wavelength, irradiance, and full-face coverage that makes this protocol practical and reproducible.