Introduction
If you have researched light therapy, you have encountered both terms: "photobiomodulation" and "red light therapy." They are frequently used interchangeably - but they are not exactly the same thing. Understanding the distinction helps you evaluate devices and evidence more accurately.
Key Takeaways
- Photobiomodulation (PBM) is the scientific/clinical term for the mechanism - light-induced biological changes in tissue
- Red light therapy is the consumer term - typically referring to at-home devices using red or near-infrared wavelengths
- All red light therapy is a form of photobiomodulation, but not all photobiomodulation uses red light (the mechanism applies across a wavelength range including NIR)
- The most important practical distinction: terms differ; the underlying mechanism and the specs that matter (wavelength, irradiance, coverage) are the same
- When evaluating devices, focus on wavelength accuracy and irradiance - not which terminology the brand uses
Are They the Same Thing?
Yes and no - and the distinction is more terminological than mechanistic.
Photobiomodulation (PBM) is the clinical/research term. It describes the biological responses that occur when specific wavelengths of light are absorbed by tissue. The term covers wavelengths from approximately 600nm to 1100nm and beyond, including visible red (630-700nm) and near-infrared (700-1100nm).
Red light therapy is the consumer-facing term. It typically refers to at-home devices using red LED light, usually 630-700nm, sometimes combined with near-infrared (800-850nm). The term is narrower in everyday usage - most consumers use it to mean visible red LED treatment.
The practical overlap: Consumer red light therapy devices operate within the photobiomodulation wavelength window. The mechanism is the same. The terminology differs by context - clinical papers use PBM; consumer brands use red light therapy.
Low-level light therapy (LLLT) is a third term sometimes used, particularly in older literature, to distinguish non-ablative light therapy from higher-power laser treatments. LLLT, PBM, and red light therapy all refer to the same category of application at consumer and clinical irradiance levels.
What the Mechanism Actually Is
Regardless of the term used, the mechanism is:
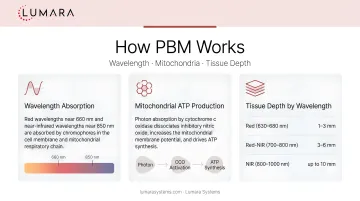
- Specific wavelengths of light are absorbed by chromophores in cells - primarily cytochrome c oxidase in mitochondria
- This absorption drives increased cellular energy (ATP) production
- Downstream effects include anti-inflammatory signaling, nitric oxide release, and support for cellular repair processes
- The depth of tissue effect depends on the wavelength - red light can penetrate approximately 5-10 mm into the skin, depending on wavelength, power, exposure time, and tissue type; near-infrared (810-850nm) reaches deeper tissue
The mechanism is the same whether you call it photobiomodulation, red light therapy, or LLLT.
What Actually Matters for Buyers
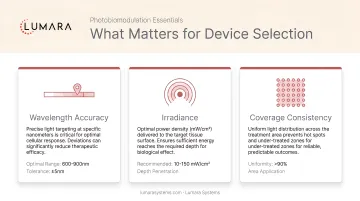
The terminology confusion is less important than the device specifications that determine whether the mechanism actually works:
Wavelength accuracy: The mechanism is wavelength-specific. A device must deliver light at the therapeutic wavelength - not just approximate it. 660nm is the most studied wavelength for skin applications; 850nm for deeper tissue. Verified output matters more than stated specs.
Irradiance at treatment distance: The amount of light energy reaching tissue per unit area per unit time. This drops with distance. Meaningful photobiomodulation requires sufficient irradiance at the actual treatment distance.
Consistency and coverage: Even distribution across the treatment area ensures all tissue receives appropriate dose.
Whether a brand calls it "photobiomodulation therapy," "red light therapy," or "LLLT" does not change these requirements.
Clinical vs Consumer: Same Mechanism, Different Scale
One distinction that does matter: clinical PBM devices used in research and professional settings operate at higher irradiance (50-500+ mW/cm²) than consumer devices (10-80 mW/cm²). This means shorter sessions in clinical settings and longer sessions at home to accumulate the same tissue dose.
This is why wavelength accuracy is even more critical in consumer devices - lower irradiance means less margin for error if the wavelength is off-target.
Frequently Asked Questions
Is photobiomodulation the same as red light therapy?
Yes, functionally. Photobiomodulation is the clinical/scientific term; red light therapy is the consumer term. Both describe light-induced cellular responses using wavelengths in the 600-1100nm range.
What is the difference between PBM and LLLT?
LLLT (low-level light therapy) is an older term for the same category of treatment. It distinguished non-ablative, low-irradiance light therapy from high-power laser procedures. PBM is now the more commonly used scientific term.
Which wavelengths are used in photobiomodulation?
The therapeutic window is approximately 600-1100nm. The most studied wavelengths are 660nm (red) for surface applications and 830-850nm (near-infrared) for deeper tissue. 660nm is the most commonly referenced for skin wellness.
Does the terminology matter when choosing a device?
No. Whether a brand uses "photobiomodulation," "red light therapy," or "LLLT," the device specs that determine effectiveness are the same: wavelength accuracy, irradiance at treatment distance, and coverage.
Same Science, Different Words
The terminology divergence between "photobiomodulation" and "red light therapy" matters for academic precision but not for device selection. The mechanism is the same; the specs that make a device work are the same.
Lumara's Illuminate V2 is built around those specs: 660nm triple-verified wavelength, 1,800 LEDs, 1,200 cm², 6,000 joules in 5 minutes, FDA cleared. Looking for help choosing between panel and mask formats? That guide covers the key differences.


