Introduction
Most explanations of red and near-infrared light therapy reference mitochondria. Fewer explain exactly what that means, why it matters, and how understanding the mechanism helps you make better decisions about devices and protocols.
This guide covers the mitochondrial basis of photobiomodulation in practical terms - enough to understand why wavelength precision matters, which tissues benefit most, and how the dose-response relationship works.
Key Takeaways
- Near-infrared and red light therapy work by stimulating cytochrome c oxidase (CCO), an enzyme in mitochondria that drives cellular energy (ATP) production
- The stimulation is wavelength-specific: 660nm and 830-850nm are the two most studied peaks of absorption by CCO
- Tissues with high metabolic demand - muscle, neurons, retinal cells, skin fibroblasts - have the most CCO and respond most to photobiomodulation
- The dose-response is biphasic: the right dose produces stimulation; too much produces inhibition (the Arndt-Schulz law)
- Understanding the mechanism explains why wavelength verification matters more than raw LED count or wattage
The Mitochondrial Mechanism
Mitochondria produce ATP - the energy currency cells use for all metabolic processes including repair, movement, and replication. The final step in ATP synthesis is carried out by cytochrome c oxidase (CCO), an enzyme complex embedded in the inner mitochondrial membrane.
CCO contains copper and heme centers that absorb light at specific wavelengths. The primary absorption peaks are:
- ~660nm (red visible light)
- ~830-850nm (near-infrared)
When photons at these wavelengths are absorbed by CCO, they:
- Increase the enzyme's activity and efficiency
- Support faster ATP production
- Release nitric oxide (NO) that had been bound to CCO, improving oxygen utilization
- Trigger downstream signaling cascades that regulate inflammation, gene expression, and cellular repair
This is why the effects of photobiomodulation extend well beyond what you would expect from simple light exposure - it is not warming tissue, it is providing a specific photochemical stimulus to the cells' energy machinery.
Which Tissues Benefit Most
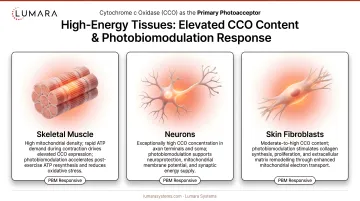
CCO is present in all cells with mitochondria, but its concentration varies significantly by tissue type. Tissues with high metabolic demand have more mitochondria and more CCO per unit volume - and therefore respond more strongly to photobiomodulation.
High-CCO tissues that respond most to photobiomodulation:
Skeletal muscle: Among the highest mitochondrial density of any tissue. Explains the strong evidence base for photobiomodulation in exercise recovery, DOMS reduction, and performance support.
Neurons: Extremely energy-intensive cells with very high mitochondrial content. Basis for research on photobiomodulation for traumatic brain injury, depression, and cognitive performance.
Cardiac muscle: High metabolic demand. Some evidence for cardioprotective effects in research contexts.
Skin fibroblasts: Moderately high mitochondrial content. Key cells for collagen production, wound healing, and skin matrix maintenance - explains the skin wellness evidence base for red light therapy.
Retinal photoreceptors: Some of the highest mitochondrial density in the body. Basis for photobiomodulation research in age-related macular degeneration and other retinal conditions.
Wavelength Windows and Tissue Penetration
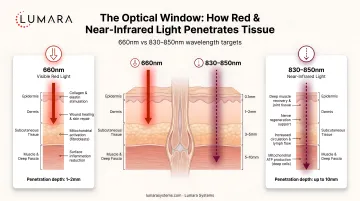
For photobiomodulation to work, the photons have to reach the target tissue. This is where the optical window concept matters.
660nm (red light): Red light can penetrate approximately 5–10 mm into the skin, depending on wavelength, power, exposure time, and tissue type. Most relevant for skin applications - fibroblasts, keratinocytes, and superficial tissue. Understanding the difference between red and infrared light therapy helps clarify which wavelength is appropriate for a given application.
830-850nm (near-infrared): Near-infrared generally penetrates deeper than visible red light, reaching muscle tissue, deeper dermal structures, and joint-adjacent areas. More relevant for muscle recovery, joint applications, and applications where deeper tissue support is the goal. Penetration varies by wavelength, power, exposure time, tissue type, and device design. For a broader overview of the near and far infrared spectrum, penetration depth differences become even more pronounced beyond 1000nm.
Outside of these windows, light absorption by water, melanin, and hemoglobin increases significantly, reducing how deep the light travels before being absorbed by non-target molecules. The 660-850nm range represents the optical window where therapeutic penetration is most practical.
The Biphasic Dose-Response
One of the most important concepts for understanding how photobiomodulation works - and why more is not always better - is the biphasic dose-response relationship (also called the Arndt-Schulz law).
At low doses, photobiomodulation stimulates cellular activity: ATP production increases, anti-inflammatory signaling increases, tissue repair accelerates.
At high doses, the same stimulus becomes inhibitory: ATP production decreases, oxidative stress increases, the therapeutic effect reverses.
The practical implications:
- Session length should follow device manufacturer guidance based on irradiance - longer is not automatically better
- Higher irradiance at shorter sessions often produces better outcomes than lower irradiance at very long sessions
- Daily sessions at the right dose outperform occasional very long sessions
- Overuse can actively reduce the benefit

What This Means for Device Selection
Understanding the mechanism clarifies what actually matters in a red light therapy device:
Wavelength accuracy is the foundation. CCO absorption peaks are at specific wavelengths. A device that claims 660nm but delivers 640nm is not stimulating the same absorption peak. Verified wavelength output - not just stated wavelength - is the most important spec.
Irradiance determines dose. The amount of light energy per unit area per unit time (mW/cm²) determines how quickly a therapeutic dose is delivered. Higher irradiance means shorter sessions for the same dose; lower irradiance requires longer sessions.
Coverage determines what gets treated. A device with high irradiance over a small area is useful for targeted treatment. A device with consistent irradiance across a large area is necessary for full-body or broad-area applications.
Consistent output over time matters. LED output can degrade with age and heat management issues. Devices with claimed lifespans and verified output stability are more reliable for long-term protocols. Unlike heat lamps, therapeutic LED panels operate at non-thermal irradiance levels - the biological effect is photochemical, not heat-based.
Lumara's Illuminate V2 delivers verified 660nm light across 1,800 LEDs and 1,200 cm², at 6,000 joules per 5-minute session. The wavelength is triple-tested, not just stated.
Frequently Asked Questions
What is the connection between near-infrared light therapy and mitochondria?
Near-infrared light at 830-850nm (and red light at 660nm) is absorbed by cytochrome c oxidase, a key enzyme in mitochondrial energy production. This stimulates ATP synthesis, nitric oxide release, and downstream anti-inflammatory and repair signaling.
Why does wavelength matter so much for red light therapy?
Because the photochemical effect is wavelength-specific. CCO absorption peaks are at 660nm and 830-850nm. Light outside these wavelengths does not stimulate CCO with the same efficiency, even if it looks similar to the eye. Verified wavelength output is more important than stated wavelength on a spec sheet.
Which wavelength is better - red (660nm) or near-infrared (830-850nm)?
Different, not better or worse. 660nm is commonly discussed for skin and superficial tissue support, with penetration that varies by wavelength, power, exposure time, and tissue type. 830-850nm generally penetrates deeper and is more relevant for muscle, joint, and neurological applications. For comprehensive treatment, both are useful.
What does "biphasic dose-response" mean for red light therapy?
At the right dose, photobiomodulation stimulates cellular activity. At too high a dose, the same mechanism becomes inhibitory. This means longer sessions are not always better - following manufacturer guidance on session length and irradiance produces more reliable results than maximizing session time.
Why do high-metabolic-demand tissues respond more to photobiomodulation?
These tissues have higher mitochondrial density and therefore more CCO per unit volume. More CCO means more capacity for photon absorption and the downstream signaling effects. Muscle, neurons, and skin fibroblasts all fall into this category.
What happens at the cellular level after a red light therapy session?
Within minutes to hours: increased ATP production, nitric oxide release supporting vasodilation, activation of transcription factors (including Nrf2 and NF-kB) that regulate inflammation and cellular stress responses. Over consistent sessions: sustained anti-inflammatory effects, collagen production support in skin cells, and accumulated tissue repair.
Mechanism First. Specs Follow From the Mechanism.
Understanding how photobiomodulation works at the mitochondrial level explains every important spec comparison: why 660nm matters, why irradiance determines dose, why coverage determines what tissue gets treated, and why consistent sessions outperform intense sporadic ones.
Lumara's Illuminate V2 - 660nm, triple-verified wavelength, 1,800 LEDs, 1,200 cm², 5-minute sessions, FDA cleared - is built around the same mechanistic foundations this guide describes.