Introduction
Near-infrared light therapy for depression and mental health is one of the more actively researched frontier applications of photobiomodulation. It is not an established treatment in psychiatry, and it is not FDA cleared for depression. But the mechanistic basis is coherent, early clinical studies are encouraging, and the research is advancing faster than in many niche photobiomodulation applications. Transcranial near-infrared photobiomodulation is an emerging research area that should not be presented as an at-home depression protocol or a substitute for psychiatric care. Anyone interested in this area should discuss it with a qualified mental health professional.
This guide covers what the science shows, what clinical studies have found, realistic expectations, and how to think about NIR therapy in the context of mental health support.
Key Takeaways
- Research on transcranial photobiomodulation uses specific near-infrared wavelengths and protocols designed to deliver light through the scalp and skull - this should not be generalized to all consumer devices
- The proposed mechanism involves mitochondrial support in neurons - relevant because neuronal energy deficits are associated with depression
- Multiple small clinical trials have shown improvements in depression symptoms with transcranial NIR therapy
- Evidence is promising but not yet definitive - large-scale RCTs are still limited
- NIR therapy is not a replacement for psychiatric care, medication, or established therapies; it is most appropriate as a complementary approach
- Consult a mental health professional before making any changes to depression treatment
Why the Mechanism Is Plausible
Neurons are among the most metabolically demanding cells in the body. They require enormous amounts of ATP (cellular energy) to maintain electrochemical gradients, neurotransmitter synthesis, and signal transmission. Mitochondrial dysfunction in neurons is increasingly associated with depression and other mood disorders.
Near-infrared at 810-850nm is absorbed by cytochrome c oxidase in mitochondria - the same cellular target as red light therapy, but at greater depth. The relevant insight for brain applications is penetration: NIR wavelengths can pass through the skull and scalp to reach cortical tissue.
Research protocols use specific device parameters to deliver NIR through the scalp. Whether consumer-level devices achieve comparable tissue doses is not yet established, and these protocols should not be assumed to translate directly to off-the-shelf consumer devices. This is the mechanistic basis for research interest in transcranial photobiomodulation (tPBM) for neurological and psychiatric conditions.
What the Research Shows
Emerging Clinical Evidence
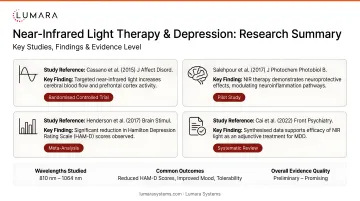
A growing body of small clinical trials and case series has examined transcranial NIR therapy for depression and other neuropsychiatric conditions:
- Several pilot studies using 810nm and 850nm NIR applied to the forehead have shown improvements in Hamilton Depression Rating Scale scores and self-reported mood measures in treated versus control groups
- Some studies have shown effects on specific depressive symptom clusters including cognitive symptoms and anhedonia
- Research at Massachusetts General Hospital (Dr. Paolo Cassano's group) has produced some of the most rigorous tPBM-for-depression work to date, with positive findings in phase II trials
Honest Assessment of the Evidence
The findings are encouraging, and the mechanistic basis is sound. The limitations:
- Most positive trials are small (20-60 participants)
- Larger phase III RCTs are underway but not yet completed for psychiatric indications
- Heterogeneity in depression subtypes makes generalizable conclusions difficult
- Consumer-level NIR devices operate at lower irradiance than research devices
- NIR therapy for depression is not FDA cleared, approved, or an established treatment
The research trajectory is positive. The evidence is not yet at the level of established psychiatric interventions.
What Research Protocols Commonly Study
Device Placement
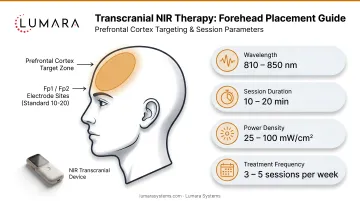
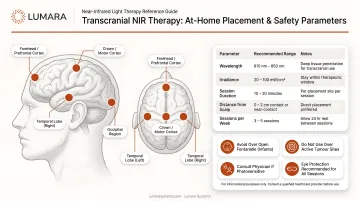
Transcranial NIR applications typically target the forehead (prefrontal cortex region) - the forehead area centered above the eyebrows and extending toward the temples. Some protocols also target the crown or posterior head. Research devices are typically applied directly to bare skin for maximum light transmission.
Session Protocol from Research
Research protocols vary, but common parameters include:
- 810-850nm wavelengths
- 10-20 minutes per session
- 3-5 sessions per week
- Protocol duration varies by study - response timelines are not yet standardized for depression-related applications
Consumer-level devices operate at lower irradiance than research devices. Whether comparable tissue doses are achievable with consumer products is not confirmed.
Important Safety and Clinical Context
- Do not modify psychiatric medications or treatment plans based on NIR therapy results without physician guidance
- NIR therapy is not a replacement for established depression treatments (medication, psychotherapy, TMS, ECT)
- Anyone with active suicidal ideation, severe depression, or complex psychiatric conditions should be managed by a mental health professional - not self-treating with light therapy
- Some research is examining tPBM for brain inflammation, post-traumatic brain injury, PTSD, and other neurological conditions - the evidence base varies by condition
How Lumara's Devices Relate to This Application
Lumara's current device lineup targets skin wellness and body recovery - not transcranial neurological or depression applications. Lumara's Illuminate V2 (660nm, 1,800 LEDs, 5 minutes, FDA cleared) delivers verified wavelength precision for surface and near-surface skin and tissue applications. It is not positioned as a transcranial NIR device, and it should not be used as a substitute for clinical depression care or as a replication of the research protocols described in this article. For users building a general wellness and recovery routine that includes red light therapy, Lumara's Illuminate V2 is a high-quality 660nm platform for those applications. Session format options such as eyes-open or eyes-closed protocols depend on the specific application.
Frequently Asked Questions
Does near-infrared light therapy help with depression?
Small clinical trials have shown improvements in depression symptoms with transcranial NIR therapy. The evidence is promising but not yet definitive - large-scale RCTs are ongoing. It is not an established treatment and should not replace medical care.
What wavelength is used for depression in near-infrared therapy?
Most research uses 810nm or 850nm NIR wavelengths applied transcranially. These wavelengths penetrate through the skull to cortical tissue.
How long does it take for near-infrared therapy to affect mood?
Research protocols typically run 8-12 weeks. Some studies show early improvements in 2-4 weeks. Individual variation is significant.
Is near-infrared therapy safe for mental health conditions?
Consumer-level NIR therapy applied externally to the head is generally considered safe for most users. Anyone with active severe depression, suicidal ideation, or bipolar disorder should be managed by a mental health professional and should discuss any complementary approaches with their treating physician.
Can NIR therapy replace antidepressants?
No. NIR therapy is a complementary approach being studied for depression support. It is not approved or validated as a replacement for antidepressants, psychotherapy, or other established treatments.
Promising Science, Appropriate Context
Near-infrared light therapy for depression has a coherent mechanism and encouraging early evidence. It is not ready to be positioned as a treatment, but it is worth following as the clinical evidence matures.
For users building a general wellness and recovery routine that includes NIR light therapy, Lumara's Illuminate V2 provides precision wavelength delivery and consistent output for daily use.