
Introduction
Peripheral neuropathy management with red light therapy requires different device thinking than skin wellness routines. The target tissue is deeper (peripheral nerves and their microvascular supply), the treatment areas are primarily extremities (feet, lower legs, hands), and the session format needs to maintain consistent contact with often awkward-to-position body areas.
This guide covers the device specifications that matter for neuropathy, why format determines effectiveness for this application, and how Lumara's Pad is built for this use case.
Key Takeaways
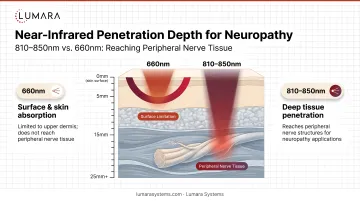
- Near-infrared (810-850nm) is the primary relevant wavelength for peripheral nerve applications - it penetrates 4-8mm to reach nerve tissue and microvascular supply
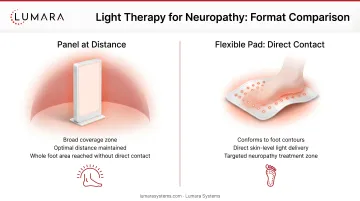
- Panel devices at a distance are impractical for feet and hands - maintaining consistent positioning during a 20-30 minute session is difficult
- Flexible pads placed directly against the extremity provide more consistent coverage than panels
- Key device specifications: verified NIR wavelength, sufficient irradiance at direct contact, appropriate size for the treatment area, and session guidance that accommodates 20-30 minutes
- If neuropathy has reduced sensation in the treatment area, you need a device with a timer and will need to monitor skin visually - you may not feel heat buildup
What the Research Shows
Clinical Evidence for Neuropathy
A 2004 study in Diabetes Care found photobiomodulation applied to the feet improved sensory measurements in patients with diabetic peripheral neuropathy. Multiple subsequent trials have shown:
- Reduced pain scores
- Improved vibration and temperature sensation in treated extremities
- Better quality of life measures related to neuropathy symptoms
Chemotherapy-induced peripheral neuropathy (CIPN) research shows more limited but positive preliminary results.
Why Near-Infrared Is the Primary Wavelength
Peripheral nerve tissue and its blood supply are located below the skin and subcutaneous tissue. 660nm red light reaches 1-4mm depth - relevant for surface tissue and skin but not consistently reaching peripheral nerve structures.
Near-infrared at 810-850nm reaches 4-8mm into tissue, accessing the small nerve fibers and capillary beds that supply peripheral nerves. For neuropathy specifically, the microvascular supply (and its photobiomodulation-driven improvement in circulation) is a key mechanism - impaired microcirculation in nerve tissue is associated with neuropathic conditions, particularly diabetic peripheral neuropathy. For a full breakdown of red versus infrared wavelength differences, see our dedicated guide. The cellular mechanism at the heart of photobiomodulation is mitochondrial ATP stimulation, which drives the downstream nerve and circulatory benefits observed in trials. For a detailed comparison of how red and near-infrared wavelengths differ, see our dedicated guide.
Why Device Format Matters
The Problem with Panels for Extremity Treatment
A panel positioned at 6-12 inches from the body works well for facial or back treatment where the body surface is flat and the user can sit or stand comfortably in front of it. For feet, it requires:
- Placing feet up toward the panel (awkward positioning)
- Maintaining that position for 20-30 minutes
- Ensuring both the top and bottom of the foot receive exposure
For lower leg or calf coverage, panel positioning becomes even more impractical.
Why Direct-Contact Pads Are Better
A flexible pad placed directly on or around the foot:
- Maintains consistent LED-to-tissue proximity throughout the session
- Can wrap over the top of the foot, ankle, and lower leg simultaneously
- Does not require maintained positioning - the user can sit or lie comfortably with the pad in place
- Can be repositioned easily between the top and bottom of the foot
What to Look for in a Neuropathy Device
Near-infrared output: Confirmed NIR wavelength (810-850nm) is the non-negotiable spec for peripheral nerve applications. Red-only devices at 660nm are insufficient for the tissue depth required. For best light absorption, apply to bare skin - no clothing or thick coverings over the treatment area. NIR light also works at the mitochondrial level to boost cellular energy in nerve tissue.
Average irradiance at direct contact: For pad-format devices, irradiance at skin contact is the relevant figure. Apply the device directly against bare skin for maximum light penetration - ask for the contact irradiance figure specifically, not just the LED spec.
Appropriate size for the treatment area:
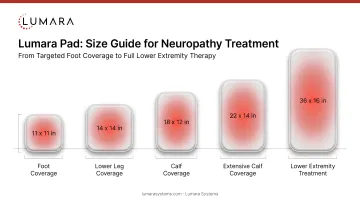
- 11x11" covers a foot and ankle
- 8x17" covers a foot, ankle, and lower leg in one placement
- Larger sizes (11x24", 12x30") cover the calf and lower leg in a single session
- Multiple passes may be needed for full lower-extremity coverage
Session time guidance: Neuropathy protocols typically require 20-30 minutes per treatment area. Devices with short maximum session times limit dose delivery.
Timer and safety features: If neuropathy has reduced sensation, you cannot rely on feeling heat buildup. A built-in timer and ability to set and forget the session are important safety features.

How Lumara's Pad Fits
Lumara's Pad combines red, near-infrared, and far-infrared wavelengths in a flexible body-contact format available in five sizes. For neuropathy applications:
- 11x11": Covers a foot and lower ankle (also useful for hand and finger coverage - see red light therapy gloves for arthritis for related device options)
- 8x17": Covers the foot and lower leg
- 11x24" and larger: For lower leg, calf, and broader extremity coverage
The 20-30 minute session guidance aligns with neuropathy protocols. The flexible format conforms to foot contours better than a rigid device. The near-infrared component provides the depth penetration relevant for peripheral nerve tissue.
The 3-year warranty reflects the build quality needed for a device used daily for months as part of a management routine.
Important Safety Note
For users with reduced sensation from neuropathy:
- Always use a timer - do not rely on sensation to determine session end (red light therapy does not generate heat the way a heating pad does, but reduced sensation still requires timer-based session control)
- Check the skin visually during and after sessions for any redness or irritation
- Start with shorter sessions (10-15 minutes) and increase gradually
- Stop and consult your physician if you notice skin changes
- Consult your physician before starting any new neuropathy treatment protocol
Frequently Asked Questions
What type of light therapy device is best for neuropathy?
A flexible pad with near-infrared (810-850nm) output that can be placed directly against the feet, lower legs, or hands. Direct contact and NIR depth penetration are the two most important characteristics for neuropathy applications. For hand and wrist neuropathy, red light therapy gloves are another format to consider.
What wavelength is best for neuropathy?
Near-infrared at 810-850nm for peripheral nerve tissue depth. Red light at 660nm contributes anti-inflammatory effects at the surface. Devices with both wavelengths provide more comprehensive coverage.
How often should I use light therapy for neuropathy?
3-5 sessions per week, 20-30 minutes per session. Consistency over 4-8 weeks before assessing response.
Why is a flexible pad better than a panel for neuropathy?
Panels require maintaining consistent positioning at a set distance from the device - difficult for feet and lower legs over 20-30 minute sessions. Flexible pads provide direct, consistent contact regardless of how the user is sitting.
Format and Wavelength Determine Effectiveness
For neuropathy applications, the device needs to deliver near-infrared wavelengths with consistent direct contact to the affected extremities. Panels designed for facial or flat-body-surface use are not the right format for this application. For users weighing red light therapy against other heat-based approaches, our comparison of red light therapy versus heating pads covers the key differences.
Lumara's Pad - NIR included, direct contact, flexible, multiple sizes, 20-30 minute guidance, 3-year warranty - is built for extremity and body recovery use.


