Introduction
Shingles (herpes zoster) causes acute viral-driven nerve pain and skin inflammation. For a significant portion of patients, pain persists after the rash resolves as postherpetic neuralgia (PHN) - one of the more difficult chronic pain conditions to manage.
Red light therapy has evidence as an adjunct for both acute shingles pain and PHN, working through anti-inflammatory and nerve-support mechanisms that are distinct from antiviral treatment. This guide covers the evidence, when to start, and how to use it.
Key Takeaways
- Shingles involves reactivation of the varicella-zoster virus in nerve tissue, causing both skin inflammation and neural damage along the affected dermatome
- Red and near-infrared light therapy reduces the neurogenic inflammation that drives shingles pain and may support nerve repair
- Some clinical studies and early evidence suggest reduced pain intensity and shorter outbreak duration with photobiomodulation alongside standard antiviral treatment
- PHN is a more persistent challenge - evidence supports light therapy for pain reduction in PHN, with sessions targeting the affected dermatome
- Red light therapy works alongside antiviral and pain management - not instead of it
- Always involve your physician in managing shingles and PHN
How Red Light Therapy Applies to Shingles
Acute Phase (During Rash)
Shingles pain has two components during the acute phase: the skin inflammation and viral-driven nerve irritation in the affected dermatome (the skin area served by the reactivated nerve).
Red and near-infrared light therapy addresses both:
- Anti-inflammatory effects on skin lesions: Red light at 630-670nm reduces pro-inflammatory cytokines and supports tissue healing in the affected skin area
- Nerve-adjacent tissue support: Near-infrared at 810-850nm penetrates to the affected nerve tract, supporting the neural tissue environment and reducing neurogenic inflammation
Postherpetic Neuralgia (After Rash Resolves)
PHN occurs when viral damage to nerve tissue produces persistent pain signal abnormalities after the acute infection resolves. This can persist for months to years and is one of the most challenging pain conditions.
For PHN, near-infrared light therapy's potential neuroprotective effects - supporting mitochondrial function in damaged nerve tissue and reducing ongoing neurogenic inflammation - are mechanistically relevant to the underlying process.
The Evidence
Acute Shingles
Some controlled studies and early evidence suggest photobiomodulation treatment during acute shingles may produce:
- Faster resolution of skin lesions
- Reduced acute pain scores
- Lower incidence of PHN development in treated versus untreated patients
The potential reduction in PHN development is particularly relevant - PHN is harder to treat than acute shingles. Some early evidence suggests PBM may help reduce the risk of PHN when used early alongside standard care, but it should not be framed as guaranteed prevention.
Postherpetic Neuralgia
Research on photobiomodulation for PHN shows:
- Significant pain score reductions in treated patients in multiple controlled trials
- Improved quality of life measures
- Effects building over consistent treatment series (typically 10-20 sessions)
PHN response varies - not all patients respond equally - but the evidence base is meaningful.

Protocol
Timing
Acute shingles: Start as early as medically cleared, alongside antiviral treatment (acyclovir, valacyclovir). Earlier treatment during the acute phase produces better outcomes for both acute pain and PHN prevention.
PHN: Sessions can begin at any time after the acute phase and are best maintained consistently over a treatment series, with response varying by severity, timing, and individual factors.
Target Area
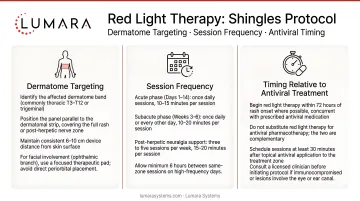
Apply treatment to the affected dermatome - the band of skin and underlying tissue served by the reactivated nerve. Common dermatomes: thoracic (chest/rib area), lumbar (lower back/hip), facial (trigeminal). The device should cover the full extent of the affected skin strip.
Session Protocol
- 10-20 minutes per session over the affected dermatome
- 3-5 sessions per week during acute phase; maintain 3x/week for PHN
- Consistent series over several weeks for PHN management, depending on symptom severity and medical guidance
- Use appropriate eye protection if treatment area is near the face (see guidance on keeping eyes open or closed during sessions)
What to Avoid
- Do not apply directly to open, weeping skin lesions during early acute phase - wait for lesion closure
- Do not use as a substitute for antiviral medication during acute shingles
- For facial/trigeminal shingles near the eye area, involve an ophthalmologist
Device Format for Shingles Treatment
Shingles and PHN affect a dermatome - a strip of skin and tissue running along a specific nerve distribution. This is typically a band across the torso, back, or hip.
A flexible pad that can be placed directly against this strip and conforms to the body contour is more practical than a panel. For thoracic and lower back dermatomes specifically, the 12x30" pad covers the affected band in most presentations.
Lumara's Pad - available in multiple sizes, with red, near-infrared, and far-infrared wavelengths - provides the direct-contact dermatome coverage that makes shingles and PHN sessions practical.
Frequently Asked Questions
Does red light therapy help shingles?
Clinical studies show photobiomodulation reduces acute shingles pain, speeds lesion healing, and may reduce PHN development when started early. It is most effective alongside antiviral medication, not as a replacement.
Can red light therapy help postherpetic neuralgia?
Multiple controlled trials show significant pain reductions in PHN with consistent photobiomodulation treatment over 8-12 weeks. Response varies by individual but the evidence is meaningful. For comparison with other nerve pain applications, the mechanisms are similar but shingles-specific protocols differ in targeting.
When should I start red light therapy for shingles?
As soon as possible after diagnosis, alongside antiviral treatment. Earlier intervention during acute shingles produces better outcomes.
Can red light therapy prevent PHN?
Some early evidence from acute shingles trials suggests lower PHN incidence in treated patients. This should not be framed as guaranteed prevention - early intervention is one reason to consider discussing light therapy as an adjunct with your physician during acute shingles.
Do I need medical supervision for light therapy during shingles?
Yes. Shingles requires medical management including antiviral treatment. Discuss light therapy as a complement with your physician. For facial shingles involving the eye, ophthalmologist involvement is essential.
Early Treatment, Consistent Protocol
For shingles, the most important variable is early intervention - the window during acute shingles is when the most significant impact on both acute pain and PHN prevention occurs.
For body-area shingles and PHN, Lumara's Pad - flexible body-contact format, red/NIR/FIR wavelengths, multiple sizes - covers the dermatome strip that shingles pain follows.