Introduction
Retinol and red light therapy are among the most well-supported tools in at-home skincare. Both support collagen production, cellular turnover, and skin quality improvement - including improvements to uneven skin tone. Both take weeks to show results. And both can cause irritation if used incorrectly.
The most common question when people start using both is: can I use them together, and if so, in what order?
The answer is yes - but sequence and timing matter. This guide covers exactly how to combine them safely and effectively.
Key Takeaways
- Retinol and red light therapy are compatible and complementary; both support collagen and cellular renewal through different mechanisms
- Do not apply retinol immediately before or after a red light therapy session - separate them by at least a few hours or use them on alternating sessions
- Red light therapy first, then retinol (if in the same routine window) is the safer sequence to avoid photosensitivity compounding
- New retinol users should introduce one product at a time before combining both - baseline tolerance matters
- Device quality determines whether red light therapy contributes meaningfully: 660nm wavelength, sufficient irradiance, and full-face coverage are the specs that matter
How Retinol and Red Light Therapy Work (and Why They Complement Each Other)
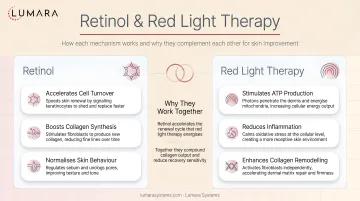
Retinol is a vitamin A derivative that accelerates skin cell turnover. It stimulates fibroblasts to produce more collagen and speeds up the rate at which dead surface cells are replaced by newer ones. The result over weeks of consistent use is improved skin texture, reduced fine line appearance, and more even tone.
The tradeoff is that increased cell turnover makes skin temporarily more sensitive - to UV, to other actives, and to physical disruption. This is why retinol users are advised to introduce it slowly and use SPF consistently.
Red light therapy at 660nm supports collagen production through a different pathway - photobiomodulation stimulates mitochondrial activity in fibroblasts, which supports cellular energy and collagen synthesis at the dermal level. It also has an anti-inflammatory effect that can reduce post-retinol irritation.
The two are mechanistically complementary: retinol accelerates surface turnover; red light therapy supports the deeper cellular activity that produces structural improvements. Used together consistently, they reinforce each other.
The Sequence Question: Which Order?
The practical concern with combining retinol and red light therapy is photosensitivity. Retinol temporarily increases skin sensitivity to light - not dramatically, but meaningfully enough that applying retinol and then immediately following with red light exposure can increase irritation risk, particularly for sensitive skin.
The recommended approach:
Option 1: Same evening, separated
- Apply red light therapy first (bare skin, no products)
- Apply retinol after your session as part of your normal evening routine
- This is the sequence most often recommended: light therapy on clean skin before product application
Option 2: Alternate sessions
- Red light therapy sessions on some evenings, retinol on others
- Reduces any compounding of sensitivity during the adaptation phase
- Preferred approach when introducing retinol for the first time or if skin is particularly sensitive
Option 3: Time of day separation
- Red light therapy in the morning, retinol in the evening
- Adds a full day's separation between the two exposures
- Works well for established routines

Timing When Introducing Both
If you are adding either retinol or red light therapy to a new routine, introduce them one at a time:
- Start with red light therapy. Use it consistently for 2-3 weeks to establish baseline tolerance.
- Then introduce retinol at a low concentration (0.025-0.05%), every other night initially.
- Once skin has adapted to both (typically 4-6 weeks), you can move to using them in the same routine using the sequence above.
This approach prevents attributing retinol purging or sensitivity to red light therapy (or vice versa) and gives you a clearer read on how your skin responds to each.
Common Mistakes
Using retinol immediately before red light therapy: Applying retinol and then immediately placing a mask on the skin before the product has absorbed increases occlusion and irritation risk. Use on clean skin or wait until product has fully absorbed.
Starting both at high intensity simultaneously: High-concentration retinol (0.5%+) combined with daily red light therapy sessions is manageable for adapted skin but risky for new users. Introduce both gradually.
Stopping red light therapy because skin is purging: Retinol causes an initial purging phase in many users. This is not caused by the red light therapy. Red light's anti-inflammatory effect may actually help manage purging severity. Do not attribute retinol adjustment to the light therapy.
Skipping SPF: Both retinol and red light therapy make skin more sensitive to UV. Daily SPF is not optional when using either consistently. This is especially relevant if combining red light therapy with other acne treatments that also increase sensitivity.
When This Combination Is Not Appropriate
- Active retinization (severe adjustment phase): If skin is actively peeling, inflamed, or highly reactive during the early retinol adjustment phase, pause red light therapy until skin has stabilized
- Open wounds or active skin conditions in the treatment area: Neither retinol nor red light therapy should be applied to broken skin
- Very sensitive or reactive skin types: Start with alternating sessions rather than same-evening use
Which Lumara Device Fits This Routine
For a skincare routine combining retinol with red light therapy, the relevant device is one built for facial use: consistent 660nm wavelength, sufficient irradiance, and full-face coverage that does not require repositioning.
Lumara's VISO LED Mask is designed for this: 660nm wavelength triple-tested for precision, 470 micro-LEDs at 30 mW/cm², 10" x 7" full-face coverage, FDA cleared. The 5-20 minute session guidance fits naturally into an evening routine - apply the mask on clean skin before your retinol application, and you have addressed both in the same session window.
Frequently Asked Questions
Can I use retinol and red light therapy on the same night?
Yes. The recommended sequence is red light therapy first (on clean skin), then retinol after your session. This prevents applying retinol under the mask and avoids any compounding of photosensitivity from the two used in immediate succession.
Which comes first - retinol or red light therapy?
Red light therapy first, then retinol. Apply the mask to clean skin before any active products. After your session, continue with your normal skincare routine including retinol.
Will red light therapy make retinol irritation worse?
No - the anti-inflammatory effect of red light therapy may actually help manage retinol sensitivity. The concern is sequencing: applying retinol before a session and then placing a mask on the skin before the product absorbs increases occlusion. Follow clean-skin, correct-sequence protocols.
How long should I wait after retinol before using red light therapy?
If you have applied retinol, wait until it has fully absorbed (15-30 minutes) before using a red light device. For the most conservative approach, alternate sessions: retinol evenings and red light evenings separately.
Do retinol and red light therapy do the same thing?
They are complementary, not redundant. Retinol accelerates surface cell turnover and has a direct retinoid receptor mechanism on skin cells. Red light therapy at 660nm supports deeper cellular energy and collagen synthesis through photobiomodulation. They reinforce each other from different mechanistic angles.
What concentration of retinol should I use when starting this combination?
Start at a low concentration (0.025-0.05%) and increase gradually. This is standard retinol introduction protocol regardless of whether red light therapy is involved. Once skin has adapted to both, you can move to higher concentrations if clinically appropriate.
Two Tools That Work Better Together
Retinol and red light therapy are both credible, evidence-supported skincare interventions. Combined correctly, they address skin quality from complementary angles - one through accelerated surface renewal, one through cellular energy and deeper collagen support.
The routine is straightforward: clean skin, red light therapy session, then retinol as part of your normal skincare sequence. Lumara's VISO LED Mask - 660nm, 470 micro-LEDs, FDA cleared, built for daily facial routines - is the device that fits this protocol.


