Introduction
Red light therapy's application to fertility is among the more discussed - and more frequently overstated - applications in the consumer photobiomodulation space. The mechanism is plausible, some evidence exists, but the clinical picture is much less clear than marketing around this topic often suggests.
This guide covers what the research actually shows, which mechanisms are supported by evidence, how to use red light therapy responsibly as part of a fertility support approach, and what realistic expectations look like.
Key Takeaways
- Red and near-infrared light therapy have a plausible mechanism for supporting mitochondrial function in reproductive cells - oocytes (eggs) are among the most mitochondria-rich cells in the body
- Direct human RCT evidence for red light therapy improving fertility outcomes is limited; most evidence comes from cell studies, animal models, and small human trials
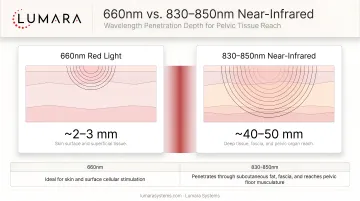
- Near-infrared wavelengths (808-850nm) penetrate more deeply than 660nm red light and are more relevant for pelvic/reproductive tissue applications
- Red light therapy should be positioned as a supportive tool used alongside - not instead of - medical fertility assessment and treatment
- Avoid pelvic red light therapy use during early pregnancy (0-12 weeks) until more safety data is available; consult your reproductive specialist
Why the Mechanism Is Plausible
Oocytes (eggs) are the most mitochondria-rich cells in the human body - they contain significantly more mitochondria than almost any other cell type. This is because fertilization and early embryo development are extraordinarily energy-intensive processes that depend on mitochondrial ATP production.
Mitochondrial dysfunction in oocytes is associated with:
- Reduced egg quality
- Poor fertilization rates
- Impaired embryo development
- Age-related decline in fertility
Near-infrared light therapy stimulates cytochrome c oxidase (CCO), the key mitochondrial enzyme involved in ATP production. For cells as mitochondria-dependent as oocytes, the logical extrapolation is that near-infrared support could contribute to improved mitochondrial health - and therefore potentially improved oocyte quality. You can read more about how infrared light therapy supports mitochondria.
This is a mechanistically coherent hypothesis. It is not yet a clinically established fact.
What the Research Shows
Cell and Animal Models
Cell studies and animal model research have shown:
- Near-infrared light therapy improving mitochondrial function in aged oocytes in mouse models
- Improved fertilization rates and embryo development quality in treated versus control groups in some animal studies
- Some evidence for protection against oxidative stress in reproductive tissue
Human Studies
Human evidence for red light therapy and fertility is limited. The most cited human study - and one that has received significant popular attention - is a Japanese study from the early 2010s examining low-level laser therapy for treatment-resistant IVF patients. That study reported improved pregnancy rates in the treated group. However:
- The study was small
- Methodology has been critiqued
- It has not been consistently replicated in larger, well-controlled trials
- It used laser devices rather than LED panels
A small number of other human studies have examined PBM for endometrial support, sperm quality, and related reproductive parameters with mixed results.
Honest assessment: The evidence base is not yet strong enough to make definitive claims about red light therapy improving human fertility outcomes. The mechanism is plausible and early signals are encouraging, but this remains a research-stage application.
How to Use Red Light Therapy as a Fertility Support Tool
For users who want to incorporate red light therapy as part of a broader fertility support approach:
Wavelength Selection
Near-infrared (808-850nm) is more relevant than 660nm red light for reproductive tissue applications. The pelvic area requires deeper penetration than red light provides at 660nm. A device with near-infrared output is more appropriate for this application.
Positioning
Lower abdomen and pelvic region (from navel to pubic bone) positions the device closest to the relevant reproductive tissue. Consistent positioning in each session is important for reproducible dose delivery.
Timing in the Cycle
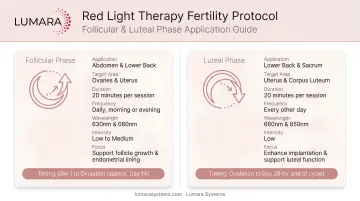
Most protocols examined in research focus on the follicular phase (days 1-14 of a typical 28-day cycle) - before ovulation, when follicle development and oocyte maturation are occurring. Some protocols also include the luteal phase.
A commonly referenced approach:
- Sessions during days 1-14 of the cycle (follicular phase)
- 5-10 minutes per session over the pelvic area
- 3-5 sessions per week
Avoid during early pregnancy (first trimester) until more safety data is available - see guidance on whether red light therapy is safe during pregnancy. If undergoing IVF or other assisted reproduction, consult your reproductive endocrinologist before starting or continuing light therapy.
Device Format
For pelvic applications, a flexible pad or panel positioned over the lower abdomen is the most practical format. Lumara's Pad - available in multiple sizes, using red, near-infrared, and far-infrared wavelengths - is designed for body-contact use over areas including the lower abdomen.
Important Caveats
This is not a substitute for fertility assessment. Anyone concerned about fertility should begin with a proper medical evaluation to identify and address underlying causes. Red light therapy as an adjunct does not replace diagnosis or treatment of conditions affecting fertility.
Avoid pelvic use during early pregnancy. The first trimester is the period of highest embryo sensitivity. Until safety data in early pregnancy is more established, pelvic red light therapy sessions should be paused once pregnancy is confirmed, and resumed only after the first trimester with medical guidance.
Male fertility: Some research has examined photobiomodulation for sperm quality, with some positive findings for sperm motility and morphology. The mechanism is the same (mitochondrial support). Men who want to explore this can discuss it with their urologist or fertility specialist.
Frequently Asked Questions
Can red light therapy improve fertility?
The mechanism is plausible - mitochondrial support in oocytes and reproductive tissue. Animal models and some early human research are encouraging. It is not an established fertility treatment and does not replace medical evaluation or treatment of fertility conditions.
What wavelength is best for fertility applications?
Near-infrared (808-850nm) penetrates deeper than red light and is more relevant for pelvic tissue. If using red light therapy for fertility support, choose a device with near-infrared output rather than 660nm red light alone.
When in the cycle should I use red light therapy?
Most research protocols focus on the follicular phase (days 1-14), when follicle development and egg maturation are occurring. Some protocols include the luteal phase. Avoid during confirmed early pregnancy.
Is red light therapy safe to use if I am trying to conceive?
Prior to conception, external pelvic red light therapy at consumer device levels is not known to be harmful. During early pregnancy (first trimester), safety data is limited - pausing is the conservative approach. Consult your reproductive specialist.
Can men use red light therapy to support sperm quality?
Some research suggests photobiomodulation may support sperm motility and morphology. The evidence is preliminary. Men interested in this application should consult a urologist or fertility specialist.
Promising but Not Proven - Use It as a Tool, Not a Treatment
Red light therapy for fertility support is an area where the mechanism makes sense and early research is encouraging, but the evidence has not yet matured to the level of clinical recommendation.
Use it as one supportive tool in a comprehensive approach - alongside appropriate medical care, lifestyle factors, and evidence-based fertility interventions. It is not a replacement for diagnosis or treatment. For a broader overview of photobiomodulation and red light therapy and PBMT therapy, those articles cover the underlying science in more depth.
For pelvic and body applications requiring near-infrared penetration, Lumara's Pad - red, near-infrared, and far-infrared wavelengths, flexible format, multiple sizes - is the most relevant device format.